AI Prior Authorization: From Administrative Burden to Automation
This article explains how AI automation eliminates the manual work in prior authorization, from real-time documentation capture to automated payer submission, so your team spends less time on hold and more time with patients.
Jaimal Soni
April 20, 2026
Why prior authorization is still a bottleneck for clinics
Prior authorization is the process of getting approval from an insurance company before delivering certain treatments, medications, or procedures. For most clinics, this means physicians and their teams spend 13 hours per week on PA, gathering records, filling out payer-specific forms, and waiting on hold to check status. AI automation changes this by capturing clinical data during the patient encounter, matching it against what each payer requires, and submitting complete requests without manual data entry.
The problem isn't that prior authorization exists. It's that the process forces your team to work across disconnected systems with incomplete information. Your front desk pulls records from one system, checks eligibility in another, fills out a form in a third, and then waits days to hear back.
Here's what this looks like in a typical clinic:
At $10.97 per manual transaction, most clinics treat this as an unavoidable cost of doing business. But it's actually a workflow problem, and workflow problems can be solved.
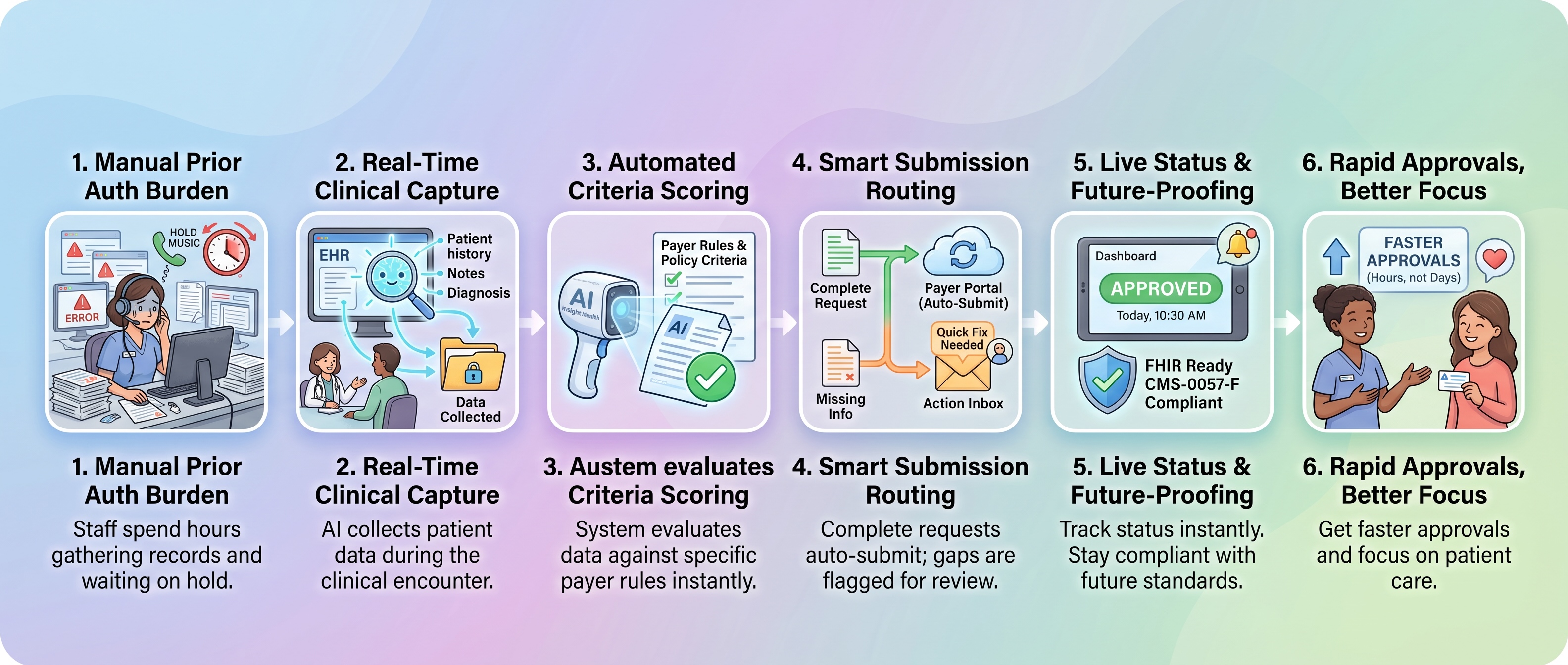
How AI automates the prior authorization workflow
I want to be clear about what AI does here. It doesn't make coverage decisions. It doesn't deny claims. What it does is capture clinical data at the moment of care and match that data against what each payer actually requires for approval.
Think of it as having a very organized assistant who knows exactly what every insurance company wants and can pull together the right documentation before anyone asks for it.
Real-time clinical data capture during the encounter
The automation starts the moment you order a service. An AI phone agent or integrated EHR tool recognizes that prior authorization is needed and begins gathering required documentation automatically.
Instead of waiting for staff to manually pull records after the visit, the system pulls relevant patient history, diagnoses, and clinical findings in real time. By the time your clinician finishes the encounter, the system already knows what the payer needs and whether you have it.
What gets captured:
This eliminates the most common reason for denials: incomplete submissions. The system knows what's missing before anyone picks up the phone.
Automated documentation scoring against payer criteria
Once clinical data is captured, the AI evaluates it against the payer's medical policy criteria. Medical policy criteria are the specific clinical conditions a payer uses to decide whether a service is medically necessary. Each payer publishes their own criteria, and they're often different from each other.
The AI reads your clinical notes and diagnostic reports, then maps what you documented to what the payer requires. If your documentation supports approval, the system flags it as ready. If something is missing, you find out immediately rather than days later when the denial arrives.
The key difference from manual processes is that your team sees the gaps before submission, not after rejection.
Intelligent submission routing and gap-fill
Once documentation is complete, the system submits the authorization request through the appropriate channel. Some payers accept electronic submissions through portals. Others still require fax or phone. An AI fax agent routes each request correctly without your staff having to remember which payer uses which method.
If critical information is missing, the system doesn't just flag it. It routes the case through intelligent branches:
Your team receives real-time status updates. No more calling payers to check on submissions. No more wondering where a request got stuck.
What prior authorization automation looks like in practice
Let me walk through a concrete example so you can see how this works in your clinic.
A patient calls to schedule a procedure that requires prior authorization. Your AI phone assistant recognizes the authorization requirement during the scheduling call and begins gathering information. It pulls the patient's recent imaging, clinical notes from their last visit, and relevant medical history. By the time the appointment is confirmed, the system has already identified what the payer needs.
The day of the visit, your clinician orders the procedure. The AI system checks the patient's current insurance, verifies that authorization is still required, and evaluates whether your documentation meets the payer's criteria. If everything is complete, it submits the request through the payer portal with zero manual data entry.
In many cases, approval comes back before the patient leaves the office.
If the payer needs clarification, the system flags it immediately. Your team gathers the additional information and resubmits the same day. No phone trees. No fax machines. No waiting a week to find out you were missing one piece of paper.
Workflow step
Without automation
With automation
Documentation gathering
Staff manually collects from multiple systems
System pulls relevant data automatically
Form completion
Staff fills out payer-specific forms
AI formats data to payer requirements
Submission
Manual upload, fax, or phone
Electronic submission through payer portal
Status tracking
Phone calls to check status
Real-time dashboard updates
Turnaround time
Days to weeks
Hours to same day
For pain management practices performing procedures like epidural steroid injections, this reduces submission time from 45 minutes to under 5 minutes. First-pass approval rates jump from the industry average of 70-80% to above 90%.
CMS-0057-F compliance and what it means for prior authorization AI
CMS-0057-FCMS-0057-F is a federal rule that requires health plans to use standardized digital pathways for prior authorization by January 2027. This matters for your clinic because the AI systems you implement today should already be built to communicate through these pathways.
FHIR APIs are the technical standard that makes this possible. FHIR stands for Fast Healthcare Interoperability Resources. It's a common language that allows different healthcare systems to share information without custom integrations.
The rule requires three specific pathways:
When you evaluate prior authorization solutions, ask specifically about FHIR PAS API readiness. You should also understand how platforms support Medicare's WISeR model, which introduces AI-assisted prior authorization for traditional Medicare Part B. A platform built on these standards means your clinic stays compliant without reworking your workflow when the mandate takes effect.
What to look for in a prior authorization automation solution
Not all prior authorization automation is the same. Some solutions just digitize the old process. A true workflow automation platform actually eliminates the manual work. Here's how to tell the difference.
Deep EHR integration, not a separate system. Your team shouldn't have to log into a separate portal to manage authorizations. The best solutions work inside your existing EHR. Authorization happens as part of your normal clinical workflow, not as an extra step your staff has to remember.
Real-time eligibility and payer connectivity. The solution should verify patient coverage and payer requirements in real time. If your system batch-processes eligibility checks overnight, you're still going to have surprises at the point of care.
Transparent criteria matching. You should be able to see exactly why the system recommends approval or flags a case for review. Avoid solutions that use historical claim data or predictive models to guess what a payer might approve. You want to know what the payer actually requires, not what worked for other patients.
Broad payer coverage. The solution should connect to national payers, but also regional and state Medicaid plans. A solution that only covers major national plans will leave gaps in your workflow. Ask specifically about the payers your clinic works with most.
Clear visibility and reporting. You need dashboards that show where authorizations are stuck, which cases are pending, and how many are being approved on first submission. This data helps you identify bottlenecks and measure improvement.
Solutions built by practicing physicians understand clinical workflows in a way that pure technology companies often miss. They know the difference between documentation that's clinically complete and documentation that's administratively complete. That distinction matters because payers reject requests that meet clinical standards but miss administrative requirements.
Frequently asked questions about prior authorization automation
Does AI prior authorization automation replace human decision-making at the payer?
No. AI automation organizes clinical information and submits complete requests, but the payer's medical review team always makes the final coverage decision. The AI is a tool to reduce manual work, not to replace clinical judgment on either side.
Will prior authorization automation work with my specific EHR system?
The best solutions use standard APIs to integrate with major EHRs including Epic, AdvancedMD, and Office Practicum. Before selecting a solution, confirm it supports your specific EHR and that integration doesn't require expensive custom development. FHIR-based solutions are more likely to work across multiple systems.
How quickly will my clinic see results from prior authorization automation?
Most clinics see measurable improvements in authorization turnaround time within the first month. Full adoption typically takes two to three months as your team adjusts workflows and the system learns your payer mix.
Does prior authorization automation eliminate the need for authorization staff?
No. It reduces the time your team spends on manual tasks like form-filling and record-gathering. Your staff still handles exceptions, complex cases, and payer communication. The goal is to free your team for higher-value work, not to eliminate positions.
What happens when a payer doesn't support electronic prior authorization submission?
A good solution has fallback pathways for manual submission and alerts your team when electronic submission isn't available. The system tracks these cases separately so you can follow up appropriately and measure which payers are creating the most friction.