Prior Authorization Approval Rates: What 2026 Data Reveals
This article breaks down what the new CMS prior authorization reporting requirements actually reveal about approval rates across Medicare Advantage, Medicaid, and ACA plans, and I walk you through practical strategies to improve your first-pass approval rates and prepare for the January 2027 electronic submission mandate.
Saran Siva
April 20, 2026
What prior authorization approval rates look like in 2026
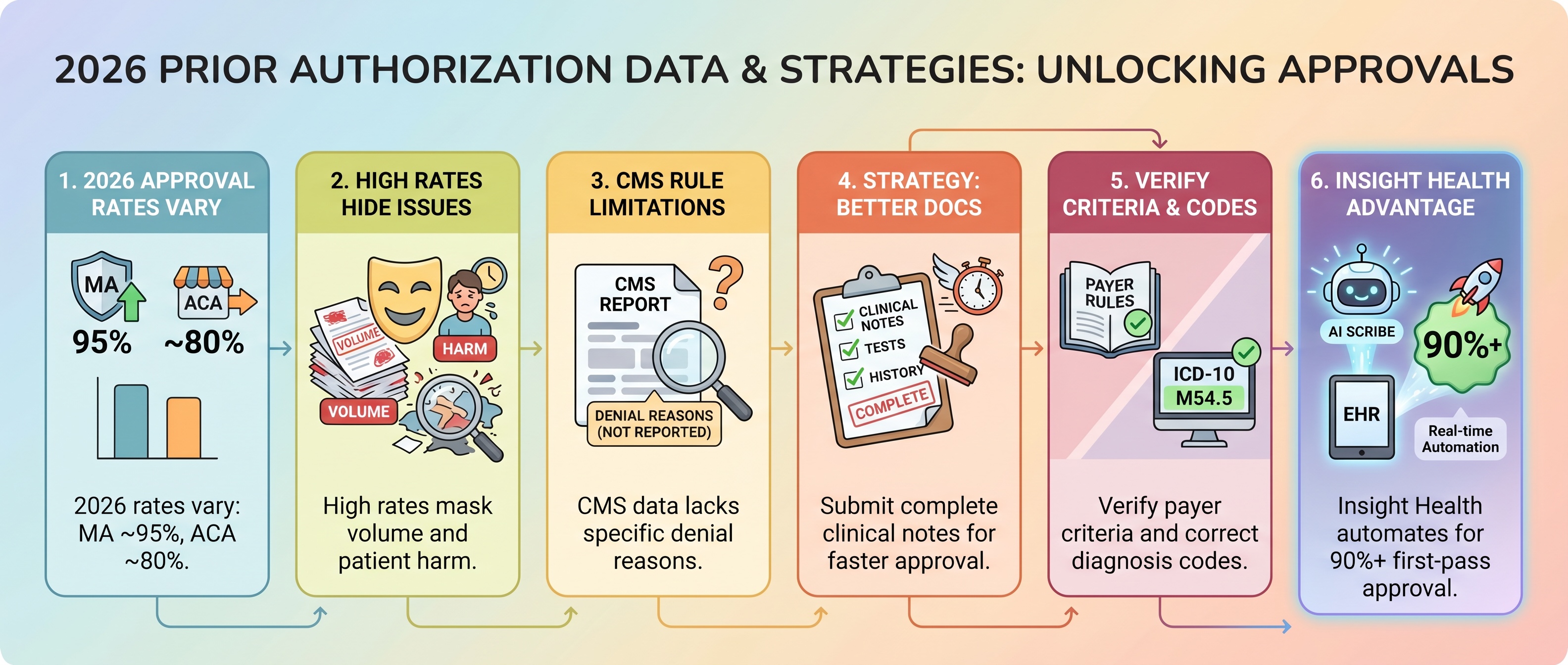
Prior authorization approval rates measure how often insurers approve requests for medical services that require advance permission. In 2026, these rates vary widely depending on the insurer and plan type. Medicare Advantage plans report the highest approval rates at around 95% after appeals, while ACA Marketplace plans show lower rates around 80%.
These numbers come from new CMS reporting requirements that took effect in March 2026. For the first time, insurers must publicly disclose their approval and denial metrics. This data reveals important differences across insurance categories that affect how you should approach prior authorization for different patient populations.
Medicare Advantage approval rates
Medicare Advantage plans report the highest prior authorization approval rates among all insurance types. UnitedHealthcare, the largest Medicare Advantage insurer, reports approximately 95% approval when including appeals. Their average decision turnaround time is 24 hours.
Only about 2.5% of Medicare Advantage claims require prior authorization at UnitedHealthcare. CMS is also piloting AI-powered prior authorization for traditional Medicare Part B through its WISeR model, which may further reshape approval workflows. The approval rate reflects a narrow slice of all services, typically high-cost procedures like inpatient hospital stays, chemotherapy, and advanced imaging.
Medicaid and CHIP approval rates
Medicaid managed care plans show approval rates in the 90% range for medical services. UnitedHealthcare reports nearly 92% approval across Medicaid and CHIP plans. This aligns with state-level data from programs like Illinois Medicaid.
Pharmacy prior authorizations tell a different story. State data from Illinois shows pharmacy approval rates dropping below 60%. The most common denial reasons include:
ACA Marketplace approval rates
ACA Marketplace plans show lower approval rates than Medicare Advantage. Some insurers report around 80% approval. This variation suggests that commercial plan standards for medical necessity differ from Medicare Advantage standards.
ACA plan approval rates are harder to compare because insurers post data inconsistently across their websites. You cannot easily find or compare prior authorization performance when shopping for plans. This makes it difficult to factor prior authorization into enrollment decisions.
Why high approval rates can be misleading
When insurers report 95% approval rates, most people assume prior authorization is working smoothly. In reality, high approval rates coexist with significant problems for physicians and patients. Understanding what these statistics hide is essential if you want to reduce administrative burden in your practice.
The aggregation problem is the biggest issue. Insurers report approval rates across all services combined. They do not break down which specific procedures, medications, or diagnoses face denials.
A 95% approval rate for "all services" could mask 80% approval for oncology treatments and 98% for routine imaging. You have no way to know which services in your specialty face the most denials.
The volume problem compounds this issue. Practices report completing 39 prior authorization requests per physician per week. Staff spend 13 hours weekly on these submissions.
Even when most requests are approved, the sheer volume creates administrative strain that pulls resources away from patient care.
The clinical harm problem is the most serious concern. More than 25% of physicians surveyed report that prior authorization has led to serious adverse events for patients. These include hospitalizations, life-threatening delays, and permanent disability.
93% of physicians report prior authorization delays access to necessary care. High approval rates fail to capture this harm.
The denial reason problem makes improvement difficult. Insurers are not required to report why requests are denied. Without this information, you cannot determine whether a denial was appropriate.
You also cannot identify patterns that would help you prevent future denials.
If 95% of requests are approved, the administrative burden may not be justified in the first place. This raises the question of whether many services should require prior authorization at all.
What the CMS prior authorization reporting rule requires
The Centers for Medicare and Medicaid Services began requiring certain insurers to publicly report prior authorization metrics in March 2026. This rule applies to Medicare Advantage plans, Medicaid managed care, CHIP, and ACA Marketplace plans. Understanding what these reports contain helps you evaluate whether publicly available data actually improves transparency.
What insurers must report
What insurers do not report
Overall approval rate for initial requests
Approval rates by specific service or diagnosis
Overall denial rate for initial requests
Reasons for individual denials
Appeal outcomes
Turnaround times by service category
Average turnaround time for decisions
Prescription drug prior authorization data
Medical items and services only
Comparison data across insurers
Finding this data presents its own challenge. Insurers post metrics inconsistently on their websites. Some require navigation to multiple pages or documents.
One insurer's website includes more than 20 individual documents detailing prior authorization rates, each representing a single contract.
To find the right data for your plan, you would need to know what contract your plan is part of. This information is knowable but not obvious. Even then, comparing across insurers requires locating the right contract on each individual insurer's website and doing some enrollment-weighted math.
Washington and Massachusetts publish more detailed prior authorization analyses. These include metrics by service category and prescription drug data. These states' approaches could serve as models for improving federal reporting requirements.
How practices can improve their own prior authorization approval rates
Rather than waiting for insurers to change their processes, you can take concrete steps to reduce denials and improve approval rates. I have identified four strategies based on patterns in the data and feedback from high-performing practices.
Complete clinical documentation before submission
Prior authorization denials often cite insufficient documentation or treatments deemed not medically necessary. Submitting a request with complete clinical notes, relevant test results, and treatment history increases the likelihood of approval on the first submission.
Your documentation should include:
Practices that submit comprehensive clinical summaries upfront see faster approvals than those that submit minimal information and wait for insurer requests for additional details.
Verify payer-specific criteria for every request
Different insurers apply different standards for medical necessity. A treatment approved by one insurer may be denied by another based on that insurer's specific clinical criteria or step-therapy requirements. Understanding insurance complexity factors in healthcare prior authorization helps you avoid preventable denials.
Check the payer's prior authorization criteria document before submitting. Confirm whether step-therapy is required, meaning the patient must fail a cheaper drug first. Verify whether the specific diagnosis code qualifies for the requested service.
For United Health Care authorization requests, their online portal provides specific criteria documents for most services.
If criteria are unclear, call the payer's clinical team before submitting. This prevents denials that result from misunderstanding requirements.
Catch ICD-10 coding errors before they cause denials
Many prior authorization denials result from incorrect or missing diagnosis codes. If the submitted diagnosis does not match the payer's medical necessity criteria, the request is denied even if the treatment is appropriate.
Verify that diagnosis codes in the EHR match the clinical documentation in the patient's chart. Ensure the primary diagnosis code reflects the condition being treated, not a comorbidity. Include secondary diagnosis codes if they support medical necessity.
When diagnosis codes change, resubmit prior authorization requests with updated codes.
Automate submission to eliminate manual data entry
Manual prior authorization submission introduces errors. Staff transpose patient identifiers, forget required fields, or submit to the wrong payer portal. Automation reduces these errors and accelerates approval.
Platforms built by physicians, like Insight Health's Prior Authorization Automation, capture clinical encounter data in real time through AI Scribe. The system automatically scores documentation against payer-specific criteria and detects ICD-10 coding errors before they cause denials. It then submits requests through payer portals with zero manual data entry.
For pain management practices performing epidural steroid injections, this approach reduces submission time from 45 minutes to under 5 minutes. The system targets 90%+ first-pass approval rates versus the industry average of 70-80%.
What the January 2027 payer mandate means for prior authorization
A second CMS mandate takes effect January 2027. Insurers must support real-time prior authorization decisions through electronic submission standards. This shift will change how you submit requests and receive decisions.
Insurers must accept electronic prior authorization submissions and provide decisions in real time or within defined timeframes. Practices using outdated submission methods like fax, phone, or mail must transition to electronic systems.
Only 35% of medical plans have fully electronic prior authorization today. Manual submission will no longer be the default.
This matters because almost half of prior authorization requests are currently submitted by phone, fax, or mail. Practices still relying on fax can reduce errors with AI fax automation while preparing for the full transition. The shift to electronic submission requires integration between your EHR, practice management system, and payer platforms.
Practices that implement automation and real-time submission capabilities before January 2027 will gain a competitive advantage. Insight Health's platform is built for CMS-0057-F compliance with FHIR PAS API readiness for the payer mandate. Practices that delay this transition risk slower approvals and increased administrative burden as the industry shifts to electronic standards.
Frequently asked questions
Recommended first-pass approval rate
Most practices should target 90% or higher first-pass approval rates. The industry average sits between 70-80%, meaning practices with strong documentation and submission processes can significantly outperform typical benchmarks.
Expected decision time under CMS rules
Under the new CMS rules, insurers must report average turnaround times. UnitedHealthcare reports 24-hour average decision times for Medicare Advantage, though complex cases may take longer and urgent requests receive expedited review.
Prescription drug PA requirements under CMS reporting
The CMS reporting rule excludes prescription drugs from public disclosure requirements. CMS-0062-P proposes extending requirements to drug prior authorizations. Pharmacy prior authorizations often have lower approval rates than medical services due to formulary restrictions and step-therapy requirements.

.png)